Surgery of the liver and pancreas has progressed tremendously in recent years. Advances in nonsurgical treatments are paralleled and in some cases outpaced, by surgical advances to problems impacting the hepatopancreatobiliary (HPB) tract, leading to growth in the population of patients with (benign and malignant) diseases of the liver and pancreas that benefit from surgery.
Complex GI surgery in general and HPBsurgery in particular requires a comprehensive, multidisciplinary approach. The use of technology is not enough to assure optimal outcome; rather, careful assessment, patient preparation/patient education and evaluation by experienced clinicians followed by proper application of therapies in an optimal sequence enable application of sophisticated surgical techniques and new technology, leading to efficient recovery and the best possible results.
There are several key surgical advances when delivered in an organized, multi-disciplinary program setting, that have expanded the population of patients who can undergo potentially curative surgical therapy for a range of HPB disorders involving these organs.
Pancreatic Surgery
Advanced Techniques and Minimally Invasive Surgery. Virtually any patient or physician becomes anxious upon discovery that there is a lesion in the pancreas, whether cyst, mass or tumor. Fortunately, markedly improved imaging, evaluation and treatment for pancreatic problems has led to a marked improvement in outcome for surgery of the pancreas and global improvement in outcome for treatment of even the most challenging pancreatic disorders.
Pancreatectomy is routinely performed in high-volume centers with a marked reduction in downtime for patients. Many operations are done to treat pancreatic disorders. Pancreatic anatomy is complex, and associated critical vascular structures are frequently involved with tumors and may require resection and reconstruction at the time of pancreatic surgery that impact resectability. As such, resection technique, reconstruction technique and minimally invasive surgical advances are examples of advanced techniques to improve outcomes for patients with pancreatic disorders.
Pancreatic Reconstruction and Vascular Resection. The whip-ple operation entails resection of the pancreatic head and thus requires resection of the duodenum (with or without a small portion of the stomach), the bile duct (and gallbladder if present), and the regional nodes. It is performed for treatment of disorders involving the pancreatic head, including pancreatic cancer, many duodenal cancers, ampullary and distal bile duct cancers.
The same anatomical procedure is performed for premalignant processes in the pancreatic head or for extrapancreatic lesions involving this area. Anatomy demands precise tissue removal made possible by precise division of the pancreas, bile duct and intestine, and dissection of the regional vessels to liberate the diseased specimen. This proper resection technique leaves the remaining stomach, bile duct and pancreas well-vascularized and disease-free ready for anastomosis to the jejunum to restore normal GI function.
The most common complication of whipple is leakage from the pancreas(pancreatic leak or fistula) reported in up to 20% of patients. Fistula rates are falling, and as technique improves, recovery time is improving as well. Experienced centers report hospitalization for whipple as little as 7-10 days, less than half the duration reported only a few years ago.
Analysis of whipple outcomes at our institution over the past several years reveals average hospitalization is only 5 days, with a < 5% pancreatic fistula rate, which results from not only experience but the aggressive, multidisciplinary planning, nutritional ‘pre-hab’ and technical surgery. (A new anastomotic technique for reconstruction of the pancreas I developed, which will soon be published in a peer-reviewed journal, likely contributes to the low fistula rate and short hospitalization.)
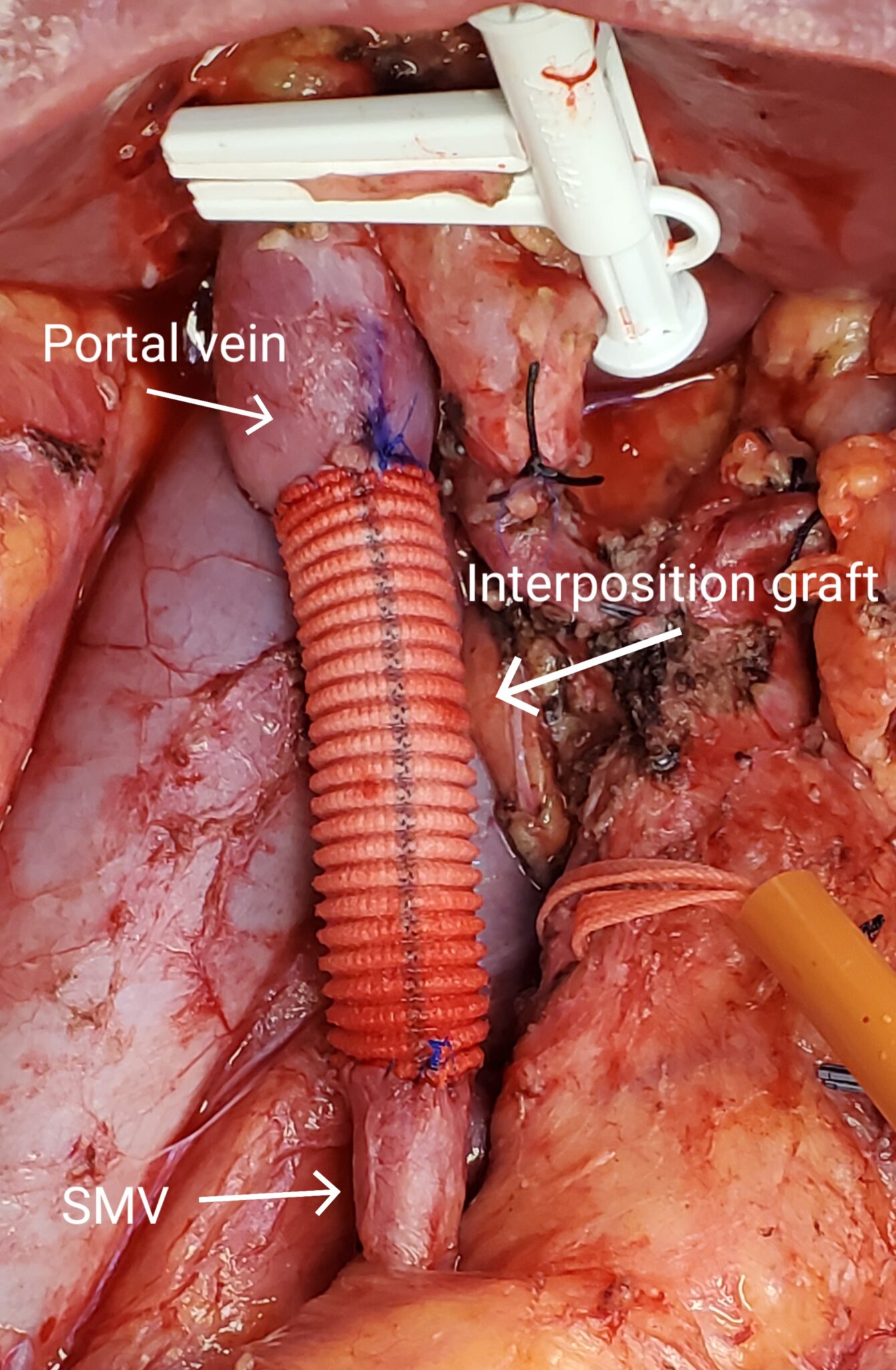
Related to pancreatic head (and tail) surgery is the critical dissection of the associated vasculature. The celiac and its branches, the superior mesenteric artery and the superior mesenteric/portal venous confluence abut the pancreas at the junction of the head and neck of the gland. Thus many disorders of the pancreatic head, particularly cancers, can involve these vessels; in appropriate patients, simultaneous resection of the pancreas with mesenteric veins (commonly) and arteries (more rarely for oncologic reasons) should be performed.
In high-volume centers, up to 20% of patients with pancreatic cancer require resection of the portal vein, with an additional proportion of patients that require en-bloc resection of either the celiac axis or its branches for curative-in-tent surgery¹. Remarkably, these patients do not experience a significant extension in hospitalization, though transfusion is more common (due to addition of vascular resection) and overall risk for complications rises modestly concordant with the additional duration and complexity of surgery. In properly prepared and operated patients, good long-term outcomes are reported, even when extensive treatment and extensive open surgery are required. (See Figure 1.)
MIS and Robotics. A second major advance for pancreatic surgery is minimally invasive surgery (MIS). Adoption is accelerating, particularly using the robotic approach². The flexibility, control and visualization with the surgical robot is well suited to pancreatectomy thanks to the wider field of surgery and dexterity of the newer-generation robots. We now perform over 60%of our pancreatectomies using the da Vinci XI robotic surgical platform. Our robotic HPB surgery volume is the highest in Georgia and in the top tier of robotic HPB programs in the U.S.
MIS pancreatic surgery started with resection of the tail. Fewer vessels to dissect and no need for reconstruction allow shorter operative times and excellent outcomes. Robotic whip-ple surgery is more in its infancy, but it is also progressing as anastomotic techniques improve. Hospitalizations are similar to open surgery and the operations take marginally longer, but progressive advances in technique are moving robotic pancreatic head surgery to the mainstream.
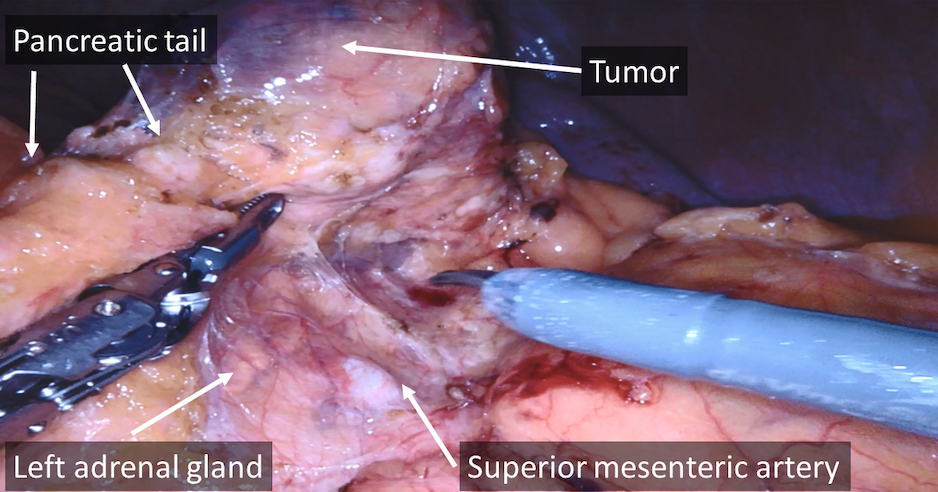
For the tail, however, outcomes are rapidly improving. Recent analysis of outcomes at our institution for distal pancreatectomy revealed reduced hospitalization by 2 days (29% reduction in hospitalization) for robotic versus open pancreatectomy. We and others have found the robotic approach allows superlative visualization of the structures to be resected and those to be preserved. Efficient robotic dissection and transection devices alongside routine intraoperative ultrasound to localize tumors and vessels al-lows radical oncologic surgery for tumors and more limited resection for benign pancreatic disorders. (See Figure 2.)
Through knowledge of anatomy, experience in conventional surgery and now years of experience with robotic pancreatic surgery, the standard of care is shifting toward minimally invasive pancreatic surgery across the country and across the globe. This is possible with the newer generation of surgical robots, which are gradually incorporating newer instrumentation that allow more complex operations to be performed with exquisite safety.
Thus technical advances such as advanced pancreatic anastomotic technique, vascular resection and reconstruction and increasingly routine robotic pancreatic surgery applied in the robust multidisciplinary environment are bringing about progressively improving outcomes for treatment of pancreatic disorders, including cancers of the pancreas requiring surgery.
Modern Liver Surgery
Liver Remodeling and MIS. Problems and challenges in liver surgery differ from those in pancreatic surgery. Specific to liver surgery is the reality that in the event of postoperative liver dysfunction, there is no ‘liver-replacement’ therapy. In contrast to pancreatic function, which can be replaced or supplemented by insulin and digestive enzyme therapy, or renal dysfunction, which can be replaced by dialysis, liver function cannot be replaced or supported effectively using current technology (short of liver transplantation, which is generally not an option). Thus efficient recovery from liver resection, especially extensive resection, requires an approach to avoid liver dysfunction.
Two ways to avoid liver dysfunction are to remodel the liver preoperatively (assure that the liver that will remain after resection will be adequate before undertaking surgery) and to minimize the stress of surgery using minimally traumatic surgical technique.
Preparing the Liver for Surgery – Liver Remodeling with Preoperative Portal Flow Diversion. A focus on complete re-section of a tumor-bearing liver expanded the use of extensive liver resection. This led to the reality that suboptimal outcomes of extensive resection were not oncologic, but linked to inadequate function of the liver that remained after resection³. As major technical complications and fatal liver failure were overcome, the limits of resection were tested with operations to remove greater proportions of liver parenchyma.
The result was cholestasis and impaired synthetic function-related morbidity with prolonged recovery in some patients, ultimately leading to the recognition that the limits of safe resection were being approached⁴. Recovery from major hepatectomy is now known to relate to the volume and quality of the liver that remains after resection (the future liver remnant, or FLR). This focus on the FLR combined with discovery of approaches to remodel the liver preoperatively – to shift volume and function away from the diseased liver toward the FLR preoperatively –exposed a new frontier in safety in extensive hepatectomy.
Standardized assessment of the liver volume and function pre-operatively is required⁵. In the event that the FLR function will be inadequate, percutaneous portal vein embolization (PVE) is indicated preoperatively. A descriptive example of PVE relates to patients with colorectal liver metastases. In the most common straightforward case, disease on the right would mandate resection of the entire right or right and central liver leaving a small, inadequate remnant (left or portion of the left) liver.
In this case, following assessment of liver volumetry and at the surgeon’s request, the interventional radiologist per-cutaneously accesses the portal branches in the liver to be resected, embolizes them, and all the incoming portal flow the liver is diverted to the healthy, disease-free FLR. Functional shift is rapid – volume increases rapidly in the first 3 to 4 weeks (and function shifts faster) so that reassessment of the FLR volume, change in volume and kinetics of volumetric change allow consideration for the same planned anatomic resection but leaving a much larger liver remnant in as little as 4 weeks post PVE.
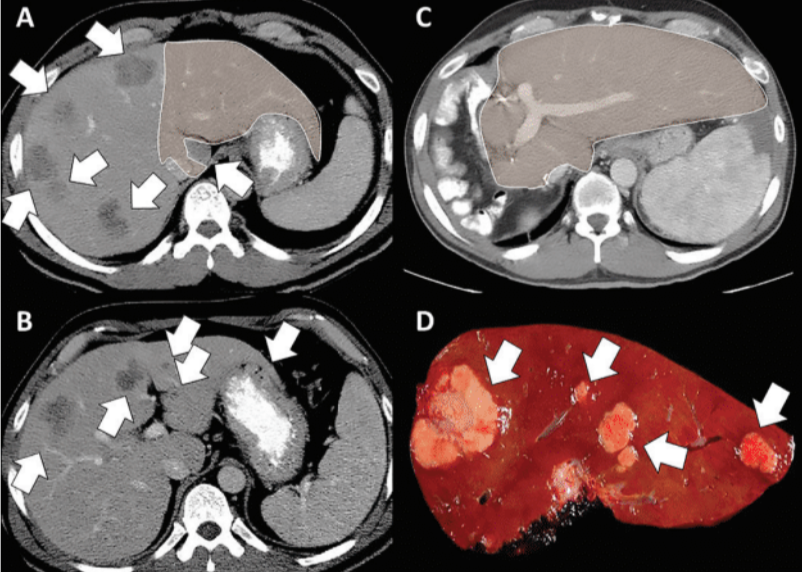
In the more complex situation, tumors are bilateral – that is, there is no disease-free FLR that can be targeted for hypertrophy (flow diversion toward tumor-bearing liver can induce tumor progression). In this case, a two-stage surgery is required.
In the first stage, the FLR is “cleaned up” by operative resection of lesions using a margin-negative but parenchyma-preserving approach within the planned FLR; disease in the remaining liver (usually the right liver) is left in place because resection of that right disease would leave the inadequate remnant. At surgery or as soon as the next day, portal flow is diverted to the newly disease-free FLR, which hypertrophies rapidly without risk for tumor progression (diseased liver is not induced to regenerate). Then at reassessment, the second-stage surgery clears of all remaining diseases safely. (See Figure 3.) This approach to two-stage surgery for colorectal liver metastases is associated with an exceptional 51% 5-year overall survival⁶. PVE is now a standard of care for extensive hepatectomy according to consensus guidelines.⁷

Robotic Liver Resection
Minimzing the Trauma of Surgery. Minimally invasive surgery has surged to the forefront of liver surgery as a method of optimal resection with minimal stress on the liver and the liver remnant. The reduction in liver manipulation, lesser impact on liver dysfunction, and flexibility and visualization of the robotic platform lead to remarkable outcomes for MIS liver resection.8 We and others have seen the impact of MIS on liver resection reflected in rapid recovery, even from substantial liver resections with low complication rates.
We recently examined our open versus robotic liver resection outcomes. Median duration of hospitalization fell from a baseline of 5 postoperative days for open hepatectomy to only 2 days for robotic hepatectomy – a 60% reduction in hospitalization over a multiyear analysis. Outcomes for resection (mainly resection of up to three liver segments) in cirrhotic patients who are at significant risk for liver dysfunction with surgery also appear to be improved with MIS vs. open surgery.9 This lesser ‘trauma’ of MIS surgery allows patients even with large lesions to undergo safe liver resection. (See Figure 4.)
Robotic hepatectomy is now moving to the mainstream. A matched cohort study published by the international robotic and laparoscopic liver resection study group investigators including 440 patients (220 matched pairs) that underwent robotic versus laparoscopic liver resection revealed a lower open conversion rate (19 of 220 [8.6%] vs 39 of 220 [17.1%]; P = .01) and a shorter postoperative hospital stay (median [IQR], 7.0 [5.0-10.0] days vs median [IQR], 7.0 [5.75-10.0] days P < .05) for robotic hepatectomy. Remarkable was the finding that after a 50-case learning curve for either technique, hospitalization remained significantly shorter following robotic versus laparoscopic hepatectomy despite a similar conversion rate to open surgery.10
Robotic approaches are now used for major hepatectomy, hepatectomy with bile duct resection, in some cases with vascular resection, and in combined liver and other GI cases. When feasible, we and others take advantage of the surgical flexibility and efficient recovery with robotic approaches to perform combined liver and colon resection for synchronous colorectal liver metastases. Quality-of-life studies suggest MIS approaches to hepatectomy significantly decrease surgical stress and comprehensive risk scores compared to open hepatectomy in cirrhotic patients.11 Prospective study of homogenous cohorts living donors with complete follow-up demonstrate higher ERAS mobility scale and body image scores following MIS versus open donor hepatectomy.12
High-quality HPB surgery requires a comprehensive, multidisciplinary, programmatic approach to assure delivery of efficient care. Focus on complete removal of diseased liver or pancreatic tumors or masses has been a central element of GI surgery and surgical oncology. Surgical advances in vascular resection and reconstruction, critical focus on patient preparation, liver preparation (remodeling, PVE) and less-traumatic approaches to surgery with robotic HPB surgery represent applications of new technology and advanced techniques, which lead to a greater proportion of patients that benefit from potentially curative liver and pancreatic surgery, with concordant reduced morbidity and improved long-term outcomes.
Multidisciplinary care that focuses on a patient-centered approach to minimize the stress of surgery through a programmatic approach will allow application of new technologies to improve patient outcomes.
References
- Younan G, Tsai S, Evans DB and Christians KK. Techniques of vascular resection and reconstruction in pancreatic cancer. Surg Clin North Am 2016 Dec;96(6):1351-1370.
- Fernandes E, Giulianotti PC. Robotic-assisted pancreatic surgery. J Hepatobiliary Pancreat Sci. 2013 Aug;20(6):583-9.
- Abdalla EK, Hicks ME, Vauthey JN: Portal vein embolization: rationale, technique and future prospects. Br J Surg 88:165-75, 2001
- Vauthey JN, Baer HU, Guastella T, Blumgart LH. Comparison of outcome between extended and nonextended liver resections for neoplasms. Surgery 1993; 114: 968-75.
- Kishi Y, Abdalla EK, Chun YS, Zorzi D, Madoff DC, Wallace MJ, Curley SA, Vauthey JN: Three hundred and one consecutive extended right hepatectomies: evaluation of outcome based on systematic liver volumetry. Ann Surg, 250:540-548, 2009
- Brouquet A, Abdalla EK, Kopetz S, Garrett CR, Overman MJ, Eng C, Andreou A, Loyer EM, Madoff DC, Curley SA, Vauthey JN: High survival rate after two-stage resection of advanced colorectal liver metastases: response-based selection and complete resection define outcome. J Clin Oncol 29:1083-90, 2011
- Abdalla EK, Bauer TW, Chun YS, D’Angelica M, Kooby DA, Jarnagin WR. Locoregional surgical and interventional therapies for advanced colorectal cancer liver metastases: expert consensus statements. HPB (Oxford). 2013 Feb;15(2):119-30.
- Becker F, Morgul H, Katou S, et al. Robotic liver surgery – current standards and future perspectives. Z Gastroenterol 2021 Jan;59(1):56-62.
- Chen PD, Wu CY, Hu RH, et al. Robotic versus open hepatectomy for hepatocellular carcinoma: a matched comparison. Ann Surg Oncol. 2017 Apr;24(4):1021-1028.
- Chong CC, Fuks D, Lee KF, et al. International robotic and laparoscopic liver resection study group investigators. Propensity score-matched analysis comparing robotic and laparoscopic right and extended right hepatectomy. JAMA Surg 2022 May 1;157(5):436-444.
- Kaneko H, Takagi S, Otsuka Y Et al. Laparoscopic liver resection of hepatocellular carcinoma Am J Surg. 2005 Feb;189(2):190-4.
- Cho CW, Choi GS, Kim JM et al. Postoperative health status and quality of life after pure laparoscopic donor hepatectomy for living donor liver transplantation. Ann Transplant. 2022 Apr 26;27:e935611.
 Eddie K. Abdalla, MD
Eddie K. Abdalla, MD
Dr. Abdalla is the founder and medical director for the Northside Hospital Cancer Institute in Atlanta, where he developed its hepato-pancreato-biliary (HPB) robotics program. He has published nearly 200 journal articles, commentaries and book chapters in addition to hundreds of abstracts and international presentations related to liver and pancreatic surgery and surgical oncology. Following a successful career at the MD Anderson Cancer Center, he became a professor and Founding Chairman of Surgery at the Lebanese American University in Beirut before joining Northside.


