Perimenopause, the transitional phase leading up to menopause, typically begins in a woman’s forties but can start earlier or later. Typically, it is the 2-7 year time before the final menstrual period. Note this does include the final year of no menses since the diagnosis of menopause is retrospectively made. Perimenopause is characterized by hormonal fluctuations that cause a variety of symptoms affecting women’s quality of life. As primary healthcare providers, clinicians play a pivotal role in recognizing, assessing, and managing perimenopausal women to optimize health outcomes during this natural but sometimes challenging phase.
Physiology and Symptoms
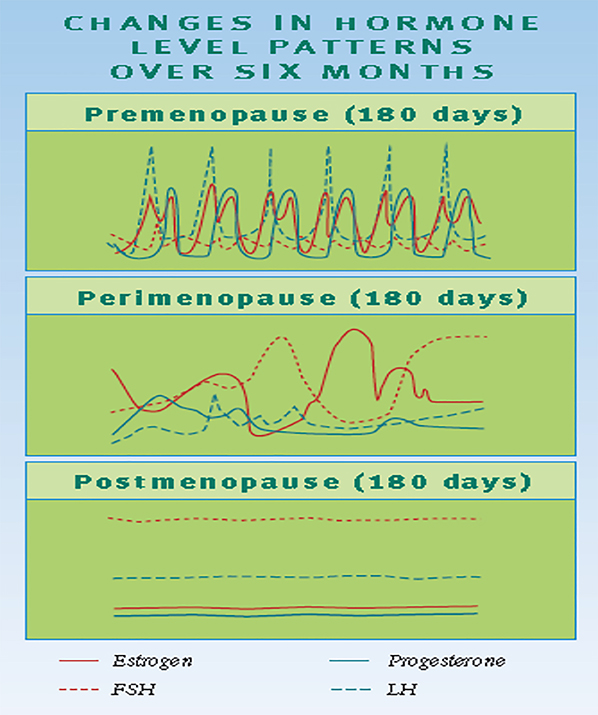
Perimenopause results from irregular ovarian follicular activity, leading to fluctuating estrogen and progesterone levels. Usually, the first indicator is a change in the interval between cycles. When cycles start to vary > 7 days, from the first day of bleeding to the subsequent cycle, perimenopause is thought to be “starting.” Menstrual irregularities may also manifest as prolonged or heavy bleeding, spotting, or irregular cycles. Abnormal uterine bleeding is a frequent concern requiring clinical evaluation and management. More specifically, during perimenopause, the ovaries gradually produce less estrogen and progesterone. The usual feedback between the ovaries, hypothalamus, and pituitary gland becomes disrupted, causing irregular ovulation or anovulation. This disruption leads to variations in cycle length and hormone levels, which can create a pattern of irregular bleeding or spotting that may appear in loops or cycles before menopause. (Harlow et al, 2012) The “loop phenomenon” in perimenopause refers to a pattern often observed in menstrual cycles during the transition to menopause. This “luteal out of phase” phenomenon occurs when an additional oocyte may be recruited early during the follicular phase, resulting in very high estrogen levels that can contribute to irregular bleeding 2 weeks after a “usual” cycle. This hormonal volatility contributes to common symptoms including vasomotor symptoms (hot flashes and night sweats), menstrual irregularities, mood changes, sleep disturbances, and urogenital atrophy (Santoro et al., 2015).
Clinical Assessment
A thorough clinical history focusing on symptom onset, pattern, and impact is foundational. Differential diagnoses such as thyroid dysfunction, hyperprolactinemia, coagulation disorders, polyps, fibroids, or malignancy must be ruled out.
Laboratory evaluations may include antimullerian hormone (AMH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol levels, though these can be variable and not diagnostic alone. Pelvic ultrasound and endometrial biopsy should be considered to exclude structural or pathological causes of bleeding if indicated. Patients with a history of polycystic ovarian syndrome (PCOS) or irregular cycles in the past or obesity with abnormal bleeding should have endometrial sampling (biopsy). Any persistent abnormal bleeding even with normal imaging (lining < 4mm) should also have further evaluation with tissue biopsy.
Management Strategies
Lifestyle Modifications
Promoting healthy lifestyle choices including regular exercise, smoking cessation, adequate sleep hygiene, and balanced nutrition forms the cornerstone of managing perimenopausal symptoms (Manson et al., 2017). Perimenopause is an opportune time to make lifestyle changes that can significantly impact a patient’s health span (not just lifespan).
Hormonal Treatment Options
Hormone therapy (HT) remains the most effective approach for vasomotor symptoms and urogenital complaints:
• Estrogen Therapy can be administered orally, transdermally, or vaginally depending on symptom profile and risk factors.
• Transdermal estrogen is preferred in women with increased risk of thromboembolism or cardiovascular disease due to its minimal first-pass hepatic effect (Canonico et al., 2007).
• Progestogen must be added in women with an intact uterus to prevent endometrial hyperplasia.
• Micronized progesterone may offer favorable safety and tolerability compared to synthetic progestins (Sitruk-Ware, 2014).
Timing and Duration: Initiation near the onset of perimenopause has increased efficacy and safety. Therapy should be individualized, using the lowest effective dose for symptom control and regularly reevaluated. In a patient who is symptomatic and still having cycles, progesterone only may help with night sweats and hot flashes, as perimenopause is in general a relative deficiency of progesterone with irregular or less functional ovulation. Also, when cycles start to space out to every 3-6 months, adding estrogen during this time can treat symptoms (along with progesterone with those who have a uterus). In other words, you don’t have to wait until the diagnosis of menopause to start hormone therapy. In fact, earlier initiation can not only treat symptoms but help decrease bone loss.
Management of Abnormal Uterine Bleeding in Perimenopause
Irregular and heavy uterine bleeding is a common challenge during perimenopause that requires targeted management to improve quality of life and rule out pathology.
• Oral Contraceptives (COCs): Low-dose combined oral contraceptives are a safe and effective option for regulating menstrual cycles, reducing heavy bleeding, and providing contraception during perimenopause. They also offer benefits such as bone mass preservation and symptom control (Speroff & Fritz, 2011).
• Levonorgestrel-Releasing Intrauterine Device (LNG-IUD): The progesterone-releasing IUD is highly effective for controlling heavy menstrual bleeding and providing endometrial protection during estrogen therapy. It is advantageous for women who prefer a long-acting, reversible option with fewer systemic hormones (American College of Obstetricians and Gynecologists [ACOG], 2018).
Both these options require evaluation and counseling regarding risks, benefits, and patient preferences.
Alternative and Adjunctive Therapies
For women who cannot or prefer not to use hormone therapy, alternatives include:
• Non-hormonal pharmacotherapies such as SSRIs, SNRIs, gabapentin, and clonidine for vasomotor symptoms.
• Cognitive behavioral therapy (CBT) has proven benefit for mood, sleep disturbances, and coping with symptoms (Freeman et al., 2014).
Patient Education and Support
Empowering women with knowledge about perimenopause normalizes their experience, reduces anxiety, and fosters adherence to treatment plans. Open communication about symptoms and treatment expectations is essential in providing holistic care.
Conclusion
Perimenopause is a significant life stage requiring attentive clinical care that addresses both physical and emotional health. Clinicians should use individualized assessment and a holistic approach, including lifestyle modification, hormonal and non-hormonal therapies, and effective management of abnormal bleeding. This comprehensive care can greatly improve the well-being of women navigating this transition.
CONTRIBUTORS
Dr. Mary Dolan is a Professor in the Department of Gynecology and Obstetrics, Emory University School of Medicine. She specializes in women’s reproductive health, menopause, and gynecologic care. Dr. Dolan earned her MD and MPH degrees magna cum laude from Emory University and completed clinical training at the University of North Carolina. She is board-certified by the American Board of Obstetrics and Gynecology and a Certified Menopause Provider. Her work includes directing reproductive health courses, engaging in research, peer review, and community outreach.
 Dr. Kawwass, Professor and REI Division Director and Emory Reproductive Center Medical Director, boardcertified in Ob/Gyn and REI, is a graduate of Davidson College, UVA Medical School, and Emory Gyn/OB Residency and REI Fellowship. She serves on the American Society of Reproductive Medicine Ethics Committee and is President-Elect of the Society for Assisted Reproductive Technology. Dr. Kawwass has published over 115 peer-reviewed publications on topics from reproductive rights to national IVF trends and outcomes.
Dr. Kawwass, Professor and REI Division Director and Emory Reproductive Center Medical Director, boardcertified in Ob/Gyn and REI, is a graduate of Davidson College, UVA Medical School, and Emory Gyn/OB Residency and REI Fellowship. She serves on the American Society of Reproductive Medicine Ethics Committee and is President-Elect of the Society for Assisted Reproductive Technology. Dr. Kawwass has published over 115 peer-reviewed publications on topics from reproductive rights to national IVF trends and outcomes.
REFERENCES
• American College of Obstetricians and Gynecologists (ACOG). (2018). Management of Abnormal Uterine Bleeding Associated With Ovulatory Dysfunction. Practice Bulletin No. 128.
• Canonico, M., Plu-Bureau, G., Lowe, G. D., et al. (2007). Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation, 115(7), 840-845. doi:10.1161/CIRCULATIONAHA.106.628164
• Freeman, E. W., Rickels, K., Lin, H., & Booth-LaForce, C. (2014). Efficacy of escitalopram for hot flashes in healthy menopausal women: a randomized controlled trial. Menopause, 21(8), 837-845. doi:10.1097/GME.0000000000000207
• Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19(4):387-395. doi:10.1097/gme.0b013e31824d8f40
• Manson, J. E., Chlebowski, R. T., Stefanick, M. L., et al. (2017). Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA, 310(13), 1353–1368. doi:10.1001/jama.2013.278040
• Santoro, N., Epperson, C. N., & Mathews, S. B. (2015). Menopausal Symptoms and Their Management. Endocrinology and Metabolism Clinics of North America, 44(3), 497-515. doi:10.1016/j.ecl.2015.05.009
• Speroff, L., & Fritz, M. A. (2011). Clinical Gynecologic Endocrinology and Infertility (8th ed.). Lippincott Williams & Wilkins.
• Stuenkel, C. A., Davis, S. R., Gompel, A., et al. (2015). Treatment of symptoms of the menopause: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 100(11), 3975-4011. doi:10.1210/jc.2015-2236
• Rossouw, J. E., Anderson, G. L., Prentice, R. L., et al. (2007). Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA, 288(3), 321–333. doi:10.1001/jama.288.3.321
• Sitruk-Ware, R. (2014). Progestogens in hormonal replacement therapy: new molecules, risks, and benefits. Climacteric, 17(Suppl 2), 1-7. doi:10.3109/13697137.2014.964646


