A healthy young woman suddenly feels her heart pounding in her chest during a stressful work meeting. She becomes lightheaded, her smartwatch shows a heart rate of 190 beats per minute, and by the time she reaches urgent care, the episode has stopped. She has had similar infrequent events before, but now they seem to be occurring more often. For many patients this is their experience with supraventricular tachycardia (SVT). While this rhythm is benign, it can be quite disruptive and alarming for those who suffer from it.
SVT is an arrhythmia originating above the ventricles. Its characteristics include a sudden onset and sudden offset, heart rate greater than 100 beats per minute and narrow QRS complexes (≤ 120 ms).
The most common mechanism is reentry, in which an electrical impulse travels in a circuit utilizing the AV node and an additional electrical connection in the heart. This extra electrical connection can be a normal variant, which leads to an arrhythmia called AV nodal reentrant tachycardia (AVNRT), or an abnormal connection called an accessory pathway, which leads to AV reentrant tachycardia (AVRT). Another common mechanism is the result of enhanced impulse formation (automaticity) that leads to focal atrial tachycardia. Atrial flutter and atrial fibrillation sometimes are considered forms of SVT and must be considered in the differential diagnosis; they tend to have different risk factors and management.
AVNRT is more common in females (67.5%)1 with onset most often between the third and sixth decade of life. The mean onset of AVRT is around age 23 and is more common in males.
Diagnosis
Patients usually present with palpitations (86%), but can also experience chest discomfort (47%), dyspnea (38%), and lightheadedness (19%). Episodes can initiate after catecholamines release during stress situations or stimulants. Symptomatic SVT may terminate spontaneously or continue until medical intervention.
A 12 lead electrocardiogram (ECG) should be obtained when possible and additional testing including Holter or event monitors may be prescribed. Wearable devices with ECG capability, such as available with smartwatch recordings, demonstrate moderate feasibility, however the accuracy is low compared to 12 lead ECG.
Management
For acute management, the success of vagal maneuvers at terminating the arrhythmia varies widely in the literature with efficacy ranging from 6-54%. When this method fails, pharmacological treatment with intravenous (IV) adenosine or a nondihydropyridine calcium channel blocker can be used.
Long term management aims not only to control the symptoms but to cure the arrhythmia, thereby avoiding recurrence. This is where the expertise of the cardiac electrophysiologist comes into play.
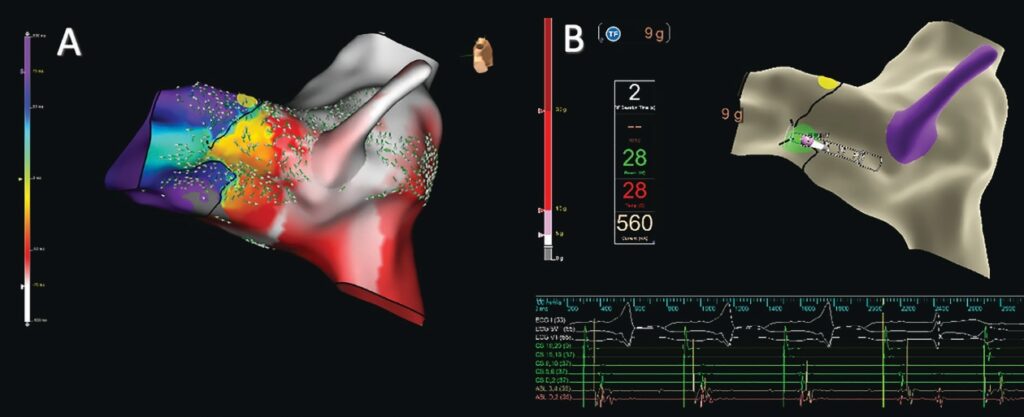
Catheter ablation of SVT is safe, cost effective and often curative of the arrhythmia. This is considered first line therapy for management of SVT. This invasive catheter-based procedure is performed in the electrophysiology (EP) lab. The procedure includes both the EP study, which is performed to diagnose the exact mechanism and location of the arrhythmia, and the ablation of the arrhythmia. Usually done under moderate sedation, the procedure involves the use of diagnostic catheters that are advanced to the heart via the femoral vein or internal jugular vein to record intracardiac electrical activity. Pacing maneuvers and mapping systems (Figure 1) can reproduce and facilitate the analysis of the arrhythmia. Once the arrhythmia mechanism is diagnosed and the locations of the electrical circuit are identified, ablation begins. This process includes delivering energy (radiofrequency, cryo-energy or pulsed electrical fields) in critical sites within the re-entrant circuit (pathway) or near the automatic focus. After confirming that the SVT is treated, patients go to the recovery area and usually are discharged the same day and can return to their regular activities the following day. Patients are asked to avoid heavy exertion for up to 1 week after the procedure.
Early referral to an electrophysiologist can prevent years of recurrent symptoms, reduce emergency visits, and eliminate the need for long-term medications. Even in patients with infrequent episodes, the possibility of sudden, severe symptoms such as syncope can justify consideration of definitive therapy.
References
- Peng G, Zei PC. Diagnosis and management of paroxysmal supraventricular tachycardia. JAMA. 2024;331(7):601-610. doi:10.1001/jama.2024.0076.
- Yalin K, Soysal AU, Ikitimur B, et al. Diagnostic accuracy of Apple Watch Series 6 recorded single-lead ECGs for identifying supraventricular tachyarrhythmias: a comparative analysis with invasive electrophysiological study. J Interv Card Electrophysiol. 2024;67(5):1145-1151. doi:10.1007/s10840-023-01695-6.
 Eduardo Quintero, MD
Eduardo Quintero, MD
Eduardo Quintero, MD, earned his medical degree from Universidad de los Andes in Venezuela. He completed internal medicine residency at Jefferson Einstein Hospital in Philadelphia, serving as Chief Resident, and cardiology fellowship at Emory University in Atlanta, where he was Chief Fellow. Now completing advanced training in cardiac electrophysiology, Dr. Quintero provides comprehensive care for heart rhythm disorders. Outside of medicine, he enjoys traveling, playing and watching soccer, and spending quality time with his family.


