Atrial fibrillation, defined as a supraventricular arrhythmia with uncoordinated activation and ineffective contraction, is the most common arrhythmia in the United States, and it continues to increase in incidence and prevalence. Two potential sequelae of atrial fibrillation are risk of stroke and significant symptoms that lower quality of life. So, in general, goals of managing atrial fibrillation include:
- decreasing the risk of stroke with appropriate anticoagulation
- reducing symptoms via rate or rhythm control strategies.
In this article, we discuss how catheter ablation has evolved as part of rhythm control strategy, and how the introduction of pulsed field energy has revolutionized management of atrial fibrillation.
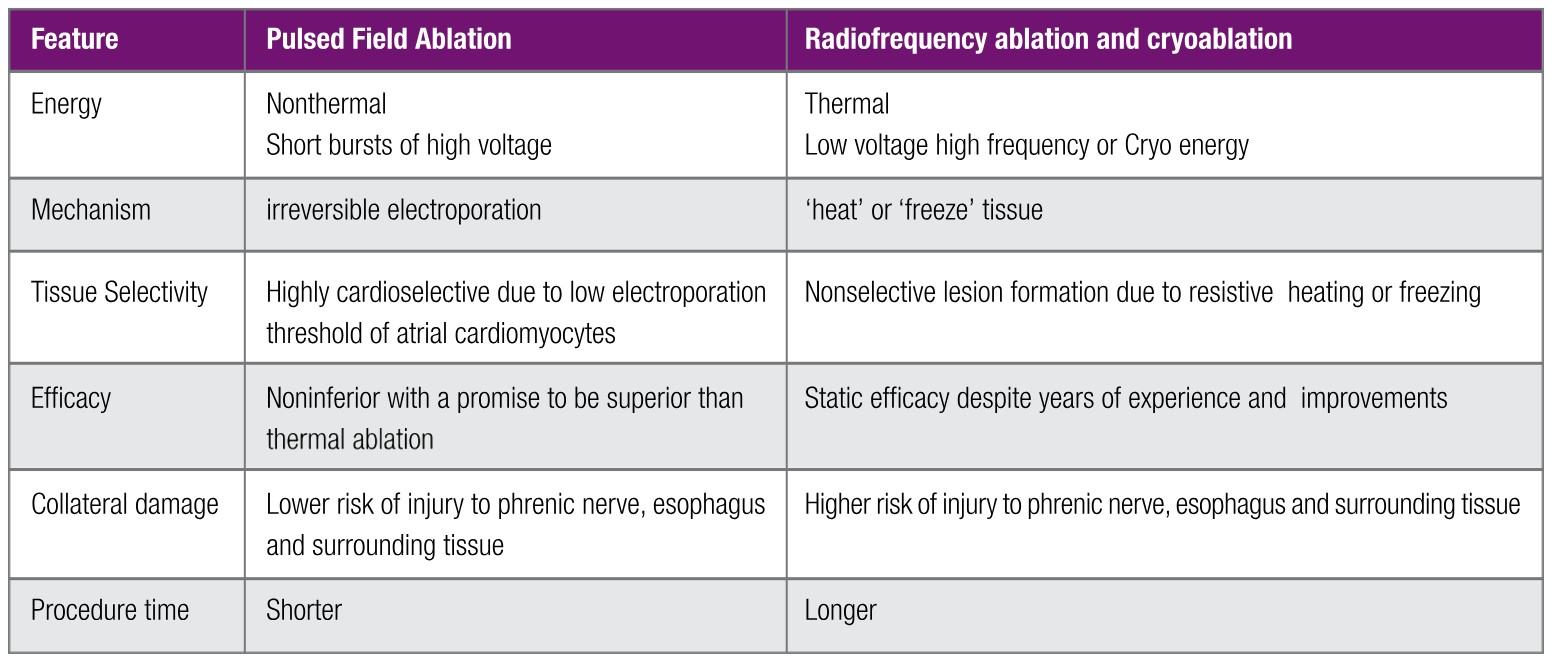
Table 1: PFA vs. Tradition Ablation
Rate Vs. Rhythm Control – Paradigm Shift
For patients with symptomatic atrial fibrillation, the preferred strategy is rhythm control that reduces afib burden and improves quality of life. Rhythm control was largely achieved with antiarrhythmic medications until the late 1990s when highly fractionated electrical signals in pulmonary veins were identified as ‘triggers’ of atrial fibrillation, and presented a clear target for catheter ablation.
In 1998, first catheter ablation of atrial fibrillation was performed using radiofrequency. In 2008, cryoballoon was introduced for afib ablation using cryoenergy. With further advances in techniques and technology, catheter ablation indeed gained more support over antiarrhythmic medications in long term management of atrial fibrillation.
And now, with the introduction of Pulsed Field Ablation, there is a paradigm shift in managing atrial fibrillation: catheter ablation can be considered a first line therapy.
Catheter Ablation with Conventional Thermal Energy and its Challenges
As discussed above, paramount in the evolution of afib management was the understanding that pulmonary veins have abnormal electrical signals that can ‘trigger’ atrial fibrillation. The goal then is to use a form of energy to cause myocyte necrosis resulting in nonconductive tissue that ‘encircles’ the arrhythmogenic substrate thereby ‘isolating’ pulmonary veins, and decreasing the probability of ‘triggering’ atrial fibrillation.
To achieve pulmonary vein isolation, radiofrequency energy is used to ‘heat’ the tissue in the antral region thus creating a ‘barrier’ and ‘trapping’ the abnormal signals within pulmonary veins. In a similar manner, cryoenergy is used to ‘freeze’ the tissue. While catheter ablation using thermal energy was a significant advancement, challenges to further progress included static long term efficacy of about 60-70%, and potential complications such as:
- damage to surrounding tissue
- atrioesophageal fistula
- phrenic nerve injury
- pulmonary vein stenosis
- atrial perforation
An innovative approach to afib ablation was clearly needed.
Catheter ablation with novel non-thermal energy: PFA and its promise
In contrast to thermal energy which causes indiscriminate tissue injury, pulsed field ablation (PFA) uses novel ‘non-thermal’ energy that is fairly cardioselective thereby limiting damage to the surrounding tissues. The mechanism is ‘irreversible electroporation’ that is accomplished by delivering short bursts of high voltage electricity that results in redistribution of charges across the cell membrane, formation of small pores, loss of cellular homeostasis culminating in rapid cell necrosis.
What makes PFA more cardioselective are the physiologic properties of atrial cardiomyocytes that have lower electroporation threshold than the surrounding structures. Therefore, delivering an electrical impulse of optimal magnitude, frequency and duration will target cardiac tissue while sparing the surrounding structures. Translating these cellular electrophysiologic properties to clinical applications has transformed the practice of afib ablation. Indeed, many studies have demonstrated the safety and efficacy of PFA which is rapidly becoming the preferred modality to achieve pulmonary vein isolation.

Figure 1 shows voltage map of pulmonary veins before (A) and after ablation (B)
While this is a novel form of energy, the actual process to deliver it is largely the same and involves catheter based electroanatomic mapping and pulmonary vein isolation. Therefore, some potential for vascular complications including coronary vasospasm persists. However, benefits are tremendous and include:
- promise of superior long term efficacy
- shorter procedure time
- lower risk of atrial perforation, atrioesophageal fistula
- lower risk of pulmonary vein stenosis, phrenic nerve injury
Table 1 summarizes features of thermal and nonthermal ablation.
Management of the most common arrhythmia has been challenging. However, with the introduction of Pulsed Field Ablation, there is a clear paradigm shift in afib management. Catheter ablation should be considered a first line therapy in most patients.
References
1. Pulsed Field or Conventional Thermal Ablation for Paroxysmal Atrial Fibrillation. Reddy Vy et. al. NEJM. 2023; 389(18):1660-1671
2. Pulsed Field Ablation: A Comprehensive Update. Ezzeddine, FM et. al. J Clin Med. 2024 Sep 1; 13(17):5191e.
 Amit D. Shah, MD, PhD
Amit D. Shah, MD, PhD
Amit D. Shah earned his MD, PhD from the University of Maryland. He completed both his Internal Medicine residency and Cardiology fellowship from the University of Medicine and Dentistry Subsequently, Clinical Cardiac Electrophysiology Residency was completed from Cedars Sinai Medical Center. Dr. Shah is board certified in Cardiology and Cardiac Electrophysiology. He is a Fellow of the American College of Cardiology and Heart Rhythm Society. He serves as the Director of Electrophysiology at St. Mary’s hospital in Athens, GA.


